Page Contents
WHAT IS IT?
The laparoscopic cholecystectomy (lap chole) is a minimally invasive surgical procedure where the gall bladder is removed.
WHY DO WE DO IT?
Patients with gall stones/cholecystitis (inflammation of the gall bladder) who are symptomatic are often the ones who undergo this surgery.
HOW DO WE DO IT?
This procedure has a few important steps that are outlined below:
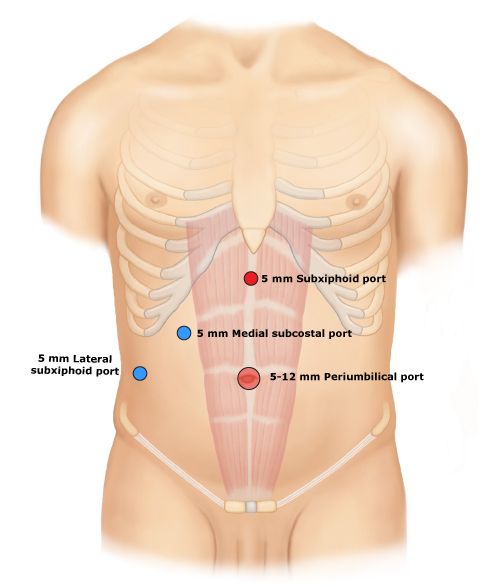
1.) Trocar placement: the first major step is to place ports so the procedure can be conducted with a laparascope.
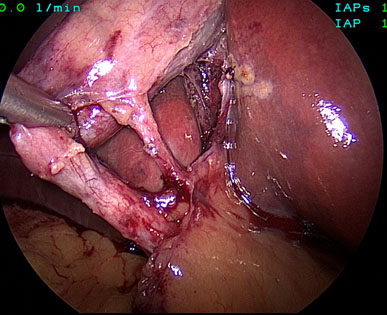
2.) Locating the gall bladder: once the ports are in place the gall bladder needs to be located using the laparoscope. Some important anatomy to appreciate (that you could be PIMPed on) is as follows:
Bowels + Omentum: a large portion of the visual field of the camera will be composed of the bowels with an overlaying fatty structure (the omentum)

Stomach: this muscular structure can be seen to the anatomical left of the liver/gallbladder.
Falciform ligament: this is the structure that connects the liver to the anterior abdominal wall and it contains the periumbilical veins.
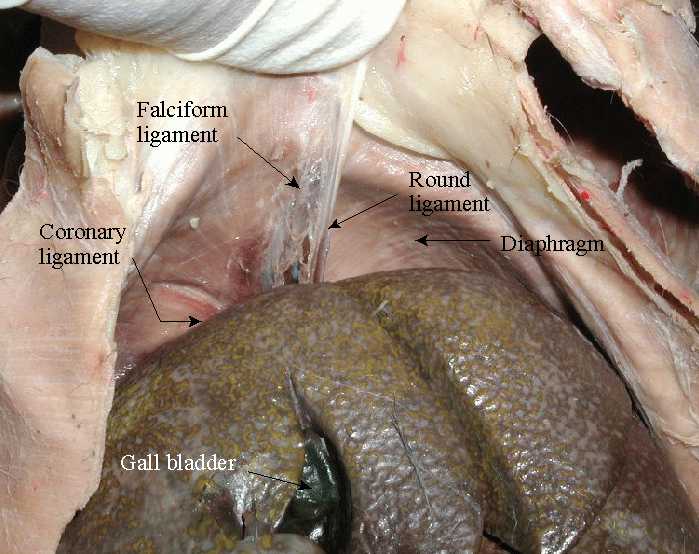
Liver and gall bladder: ultimately it will be very important to find the laparoscope that is inferior to the liver.
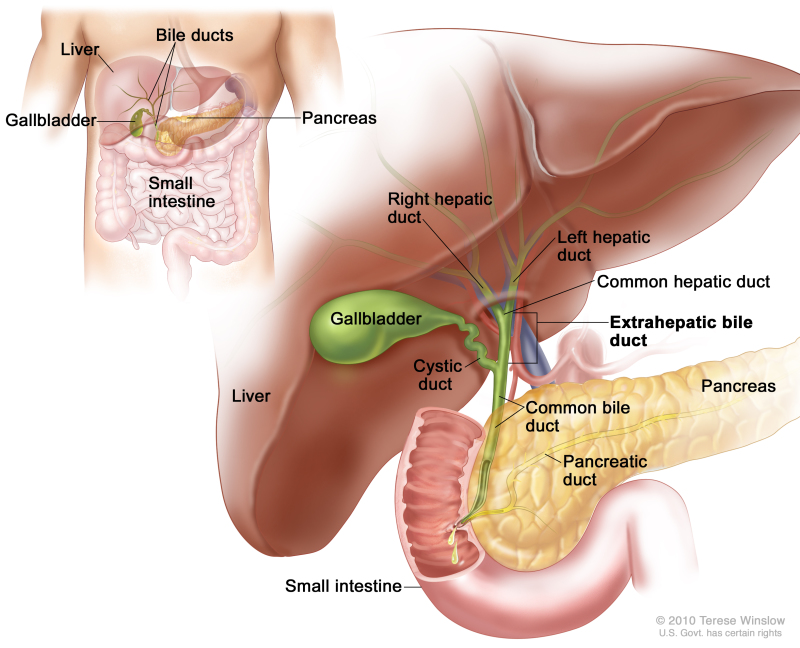
3.) Obtain critical view of safety: this refers to dissecting around the gall bladder such that both the cystic duct and cystic artery are clearly exposed (separated form other structures) and the only structures that are going into the gall bladder. The liver base should also be able to be visualized.
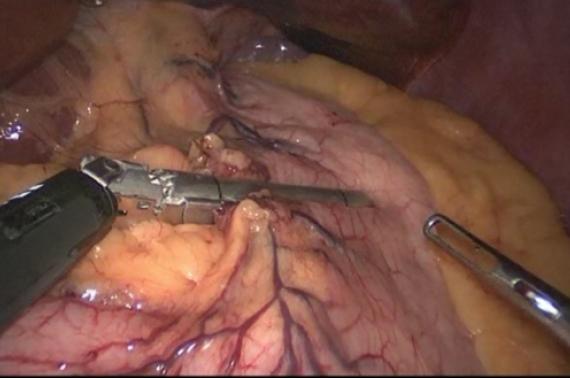
4.) Clip and cut the cystic duct/artery: once the cystic artery and duct are exposed clearly, they both can be clipped and cut so that the gall bladder can be removed. Typically 2 clips are placed on the side of the duct/artery that remains in the patient, and one clip on the side that is removed.
5.) Detachment of gall bladder from the liver: it is important to keep in mind that the body of the gall bladder is fused with the liver, and must be removed in order for the procedure to be completed. Once the gall bladder is free from the liver, it can be removed through one of the trocars.
6.) Closing: once the procedure is completed, the port sites need to be closed. Typically most of these port sites can be closed with a single buried stitch.
WHAT ARE SOME POSSIBLE COMPLICATIONS?
Cutting the common bile duct can occur if the critical view of safety is not properly obtained. It is important to remember that the common bile duct does not need to be visualized to complete this surgery, and it should not be damaged in any way.
OTHER INFO
Page Updated: 04.13.2016