Page Contents
OVERVIEW
This page is dedicated to covering a very important call case: closed loop small bowel obstruction. This page will specifically cover this diagnosis in the setting of making the finding on abdomen/pelvis CT imaging.

Many of the cases presented here will be CT scans of the abdomen/pelvis with contrast however certain cases may present non-contrast imaging (which can have overlapping findings).
WHAT IS IT EXACTLY?
A closed loop bowel obstruction is a subtype of small bowel obstruction (SBO) where a portion (loop) of the small bowel is obstructed in isolation from a mechanical cause. In many cases this is caused by an internal hernia, however the terms are not identical as other etiologies can cause a closed loop SBO, and not all internal hernias will cause a closed loop obstruction.
The implication of calling a closed loop is that there is more that one transition point which excludes the affected loop from the rest of the GI system and has caused (or will shortly cause) vascular compromise similar to a compartment syndrome (usually by restricting venous outflow).
WHY IS IT AN IMPORTANT CALL CASE?
A closed loop small bowel obstruction can be a very time sensitive and clinically impactful finding. Given the high likelihood that the closed off loop of bowel will become ischemic (and eventually) necrotic, the sooner this finding is made the higher chance the patient has to avoid requiring a bowel resection.
WHAT CLINICAL CONTEXT HELPS RAISE SUSPICION FOR THIS DIAGNOSIS?
Patients who present with clinical signs and symptoms of small bowel obstruction can raise concerns for this diagnosis (any patient who has a SBO might have a closed loop in theory). Notably no single part of the workup is incredibly sensitive or specific for diagnosing SBO however the constellation of findings can be useful. Couple clinical details to keep in mind:
- Chief complaint: abdominal pain, abdominal distention, vomiting/nausea, lack of passing gas or stool
- Relevant medical history: any prior history of abdominal surgery is a risk factor for developing SBO (and can also be a risk factor for an internal hernia/adhesions that could potentially cause a closed loop SBO).
- Unstable vitals: while not a requirement, patients with a closed loop (particularly those with ischemia/necrosis) can have vital sign abnormalities such as tachycardia and hypotension.
- Elevated white count/lactate: patients with an elevated white count may have significant bowel inflammation and those with an elevated lactate could also have bowel ischemia. These are non specific lab values but can be concerning.
WHAT IS THE KEY TO MAKING THIS DIAGNOSIS ON CALL?
There are a few imaging features to keep in mind when making this diagnosis. It is important to realize that this is a MECHANICAL diagnosis and additional features of bowel inflammation/ischemia (while common) are not REQUIRED to make the diagnosis. The below video playlist summarizes these findings and applies them to various cases from the associated case archive.
There Must Be a Small Bowel Obstruction:
While this may appear simple, it is worth stating that one can’t have a closed loop SBO without the actual SBO. For this reason, when diagnosing a closed loop the first step is to identify evidence of a small bowel obstruction. Often times the clearest sign will be the presence of both large caliber (distended, fluid/stool filled bowel) and decompressed bowel within the abdomen.
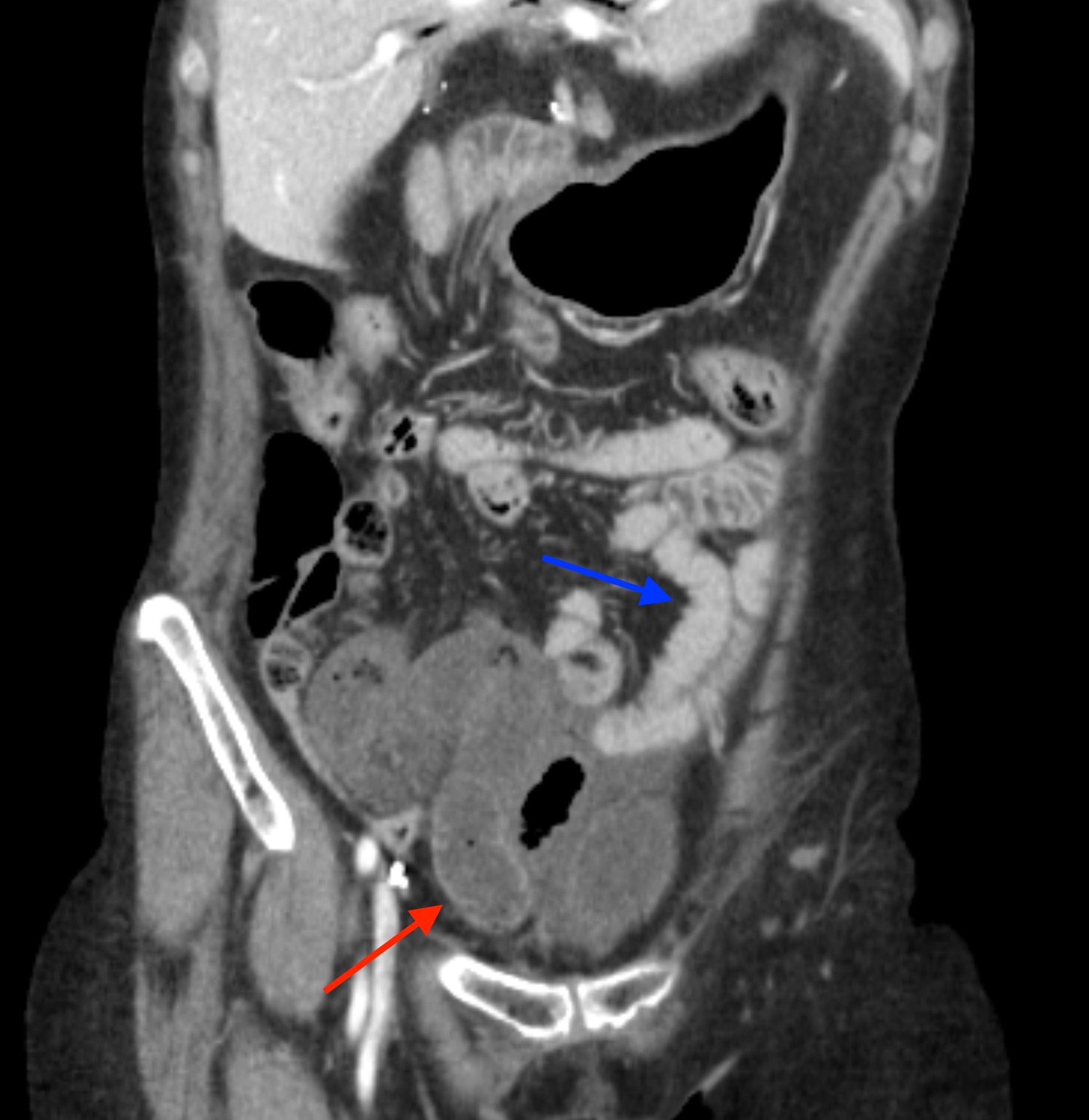
Even before a potential transition point is identified, seeing both types of bowel (with differing calibers) should help the viewer realize they are likely dealing with some sort of small bowel obstruction.
Two (Or More) Transition Points (“Closed Loop” Pathology):
Once a small bowel obstruction is identified, it is always good practice to try and find the “transition point”, where the bowel caliber changes from large/distended to small/decompressed. It is at this point where (for every SBO case) one should look to see if there is more than one transition point affecting the same portion of distended bowel.

If there are two (sometimes more) transition points affecting the same portion/loop of bowel, we have reached the threshold to call a closed loop SBO.
Obstruction Isolating a Loop Of Bowel:
In some instances the transition points may be challenging to definitively see, however there are imaging findings that might suggest that a loop of bowel is “closed” and that the SBO is only affecting this lone loop of bowel (which can suggest the diagnosis of closed loop “SBO”). Here are some imaging features to look out for:
“Balloons on a string” appearance: some closed loop small bowel obstructions demonstrate this characteristic finding where a slice of the CT scan shows distended bowel loops that all emanating from the point of obstruction, looking similar to a group of balloons held by strings. This is made more pronounced by mesenteric edema.
Isolated portion of distended bowel: if only a short segment of bowel is involved/distended one must ask why? This can be a sign that a loop of bowel is closed off from the rest of the GI tract.
Decompressed bowel proximal and distal to affected loop: this is similar to some of the above findings, however sometimes it is hard to appreciate exactly what is proximal/distal to the affected (dilated) small bowel loop. Regardless, if this is seen it is a very suspicious sign that there is a closed loop present.

Signs of Bowel Compromise/Ischemia:
While not necessary for making the diagnosis (as early closed loop SBO can be caught before there is ischemic bowel) it is important to look for signs of vascular compromise affecting the bowel. These findings can also help raise suspicions for closed loop (if one was thinking of “letting go” the idea that the case might be a closed loop. Findings of bowel compromise include (but are not limited to):
- Poorly enhancing/non-enhancing bowel wall: this can be the case in the setting of bowel necrosis or ischemia.
- Bowel wall inflammation/edema: thickening and associated fat stranding can be suggestive of ischemic inflammation.
- Mesenteric inflammation/edema: often times in the case of closed loop, the mesentery will also become ischemic which can manifest in mesenteric fat stranding/edema that appears in a segmental distribution (i.e. the segment associated with the bowel that is compromised).
- Bowel wall hyper-enhancement: this can be seen in the setting of re-perfusion injury and or bowel wall hemorrhage
Swirling Mesentery Sign:
While not all cases of closed loop are caused by internal hernias, many are. In some instances swirling of the mesenteric vessels/fat can be appreciated on imaging (at the site of the hernia) which can be suggestive of the underlying pathology. This finding is best seen in the associated scrollable cases/case discussion videos.
WHAT HAPPENS NEXT AFTER THE DIAGNOSIS IS MADE?
After this diagnosis is made, in most cases the patient will be taken to the operating room so that the closed loop obstruction can be addressed. This is what makes this call so clinically impactful as it directly affects management. Not all cases of SBO require surgery for resolution, however the implication of a closed loop obstruction is that it will require surgery for treatment, and if left alone, will result in the death of bowel.
CASE ARCHIVE
Use the following login information to access the case archives: USERNAME: user, PASSWORD: password.
Click here to open up a case archive of closed loop small obstruction cases seen on CT.
Page Updated: 11.16.22