Page Contents
OVERVIEW
This page is dedicated to organizing various examples of standardized exam questions whose answer is achalasia. While this may seem a odd practice, it is useful to see multiple examples of how achalasia will be characterized on standardized exams (namely the boards and the shelf exams). This page is not meant to be used as a traditional question bank (as all of the answers will be the same), however seeing the classic “test” characterization for a disease is quite valuable.
KEY CHARACTERISTICS OF THIS CONDITION (ON EXAMS)
When it comes to standardized exams, each topic has its own “code” marked by key buzzwords, lab findings, clues, etc. If you are well versed in this code you will be able to more quickly identify the condition that is being discussed, and get the right answer on the exam you are taking. Below is the “code” for achalasia.
- Persistent dysphagia of both solids and liquids (patients may even have weight loss due to inability to eat).
- Bird beak esophagus: on a barium swallow (seen in the context of a dilated esophagus)
- Increased resting tone of the lower esophageal sphincter can be deleted on esophageal manometry (LES does not relax).
QUESTION EXAMPLES
Question # 1
A 55 year old woman comes to the clinic because she has been having difficulty swallowing for the past year. She explains that the symptoms have been getting worse, and now sometimes she will also vomit up undigested food. She explains that she has a cough that is more severe at night as well. She has lost 15 lbs over the past 5 months. She denies any pain with swallowing or speaking. Her past medical history is non-contributory and she does not take any medications. Her temperature is 98.7°F, pulse is 75/min, respirations are 20/min, and blood pressure is 120/85 mm Hg. A physical exam is unremarkable. A chest X-ray reveals the presence of an air-fluid level at that posterior mediastinum at the level of the cardiac silhouette. Manometry shows a normal lower esophageal sphincter pressure and no relaxation of the lower esophageal sphincter when the patient swallows. What is the diagnosis in this patient?
Explanation # 1
No relaxation of the lower esophageal sphincter when the patient swallows = achalasia
Question # 2
A 50 year old woman describes difficulty swallowing which she has had for many years. She says that liquids are more difficult to swallow than solids. She has learned to sit up straight and wait for the fluids to go down her throat. Occasionally she regurgitates large amounts of undigested food. What could the diagnosis be in this patient?
Explanation # 2
Difficulty swallowing = achalasia should be considered (other diagnosis also possible, depends on answer choices available).
Question # 3
A 45 year old male complains of retrosternal discomfort and difficulty swallowing. He smokes 1 pack of cigarettes a day and drinks a 6-pack of beer regularly on the weekends. His BMI is 34.3 kg/m³. Esophageal manometry is performed and demonstrates an increased resting pressure of the lower esophageal sphincter. What si the diagnosis in this patient?
Explanation # 3
Increased resting pressure of the lower esophageal sphincter = achalasia
Question # 4
A 40 year old male with Chagas disease presents to the ED with a 3 hour history of moderate chest pain. He has lost 5 lbs in the past 2 months. His vitals are as follows: HR is 105 bpm, respirations 22/min, blood pressure 140/80 mm Hg, and O2 sat of 97%. An EKG is performed and is unremarkable. A barium swallow reveals a dilated esophagus with a “beak-like” narrowing of the at the level of the lower esophageal sphincter. What is the likely diagnosis in this patient?
Explanation # 4
Bird beak esophagus on barium swallow = achalasia
Question # 5
A 40 year old female comes to the clinic complaining of difficulty swallowing solids and liquids for the past 4 months. She explains that during this time she has lost 6 lbs. She has smoked 2 packs of cigarettes daily for the past 15 years. Her vitals are all within normal limits. Her physical exam is non-contributory. And upper endoscopy is notable for retained secretions in the esophagus, however no other pathology is noted. Results of a barium swallow are shown below.
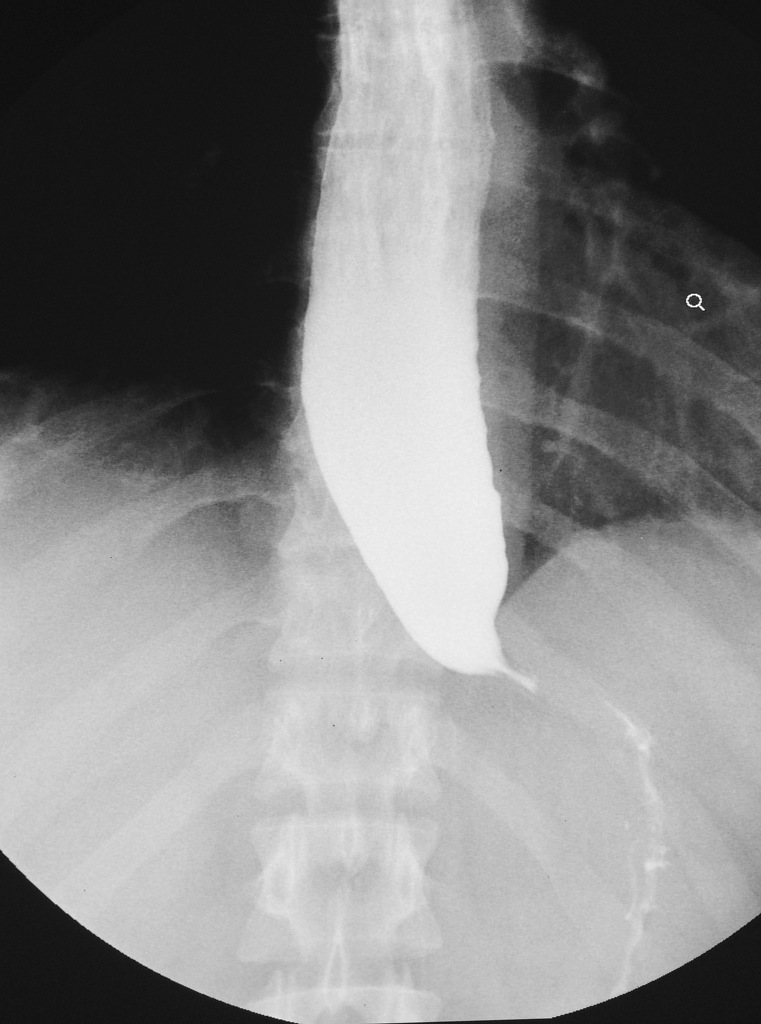
Explanation # 5
Bird beak esophagus on barium swallow = achalasia
Question # 6
Explanation # 6
TESTABLE FACTS ABOUT THIS TOPIC (BEYOND ITS IDENTIFICATION)
Many questions on standardized exams go beyond simply recognizing the underlying topic. Often there are specific testable facts regarding some aspect of the topic’s pathophysiology/management/clinical implications that are commonly asked. Some of these are listed below:
- Expected manometry findings:
- Decreased esophageal peristalsis
- Increased lower esophageal sphincter tone
- Cause: failure of the lower esophageal sphincter to relax due to the loss of the myenteric (Auerbach) plexus. These neurons are inhibitory and contain NO that normally would relax the LES. In other words: reduced numbers of inhibitory ganglion cells present in the esophageal wall.
Page Updated: 01.22.2017