Page Contents
OVERVIEW
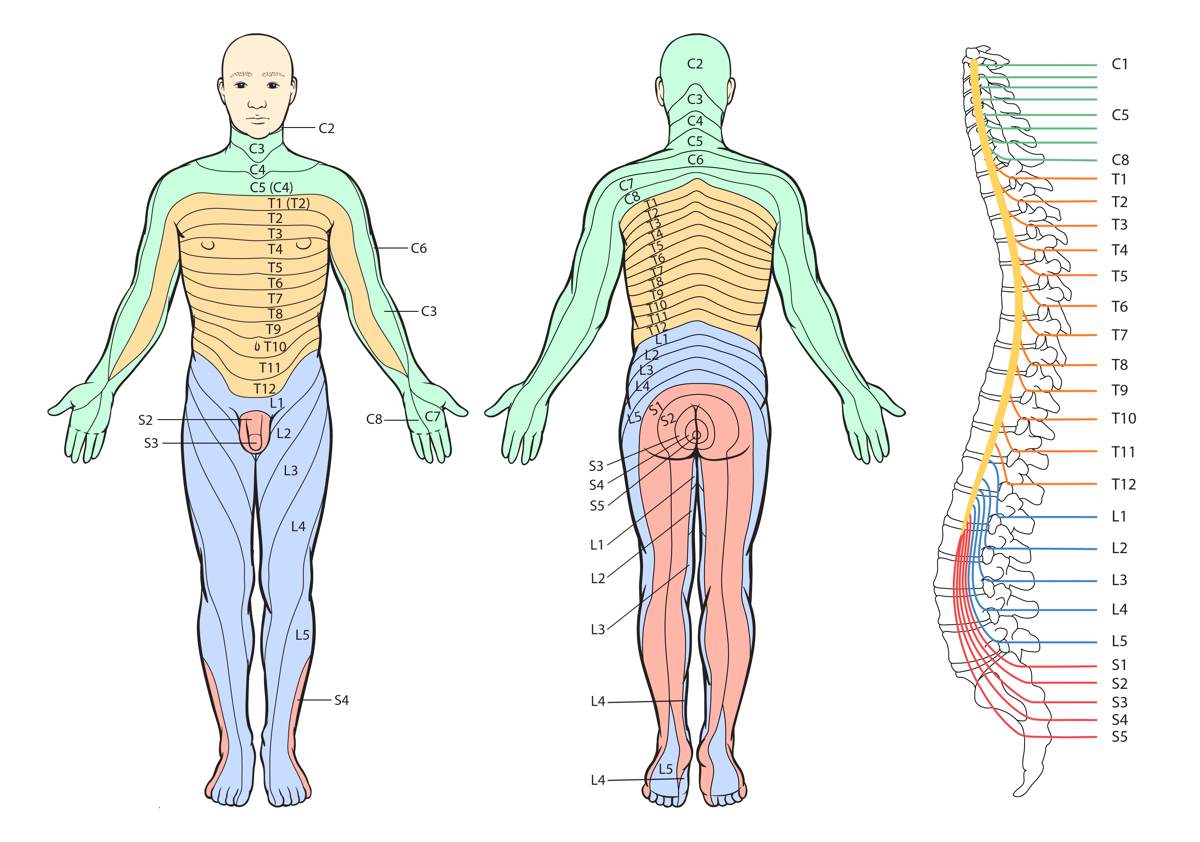
This page is dedicated to covering the sensory dermatomes of the body. All to often students learn these dermatomes only to forget them soon after they are memorized. To try and break this pointless cycle this page organizes all of the dermatomes (and their clinical significance) in a easy to reference manner.
WHAT ARE DERMATOMES?
In the realm of neurology, a dermatome refers to an area of skin that is innervated by a single spinal nerve. These areas of skin carry sensation (and the perception of pain) from the associated region to the brain for processing.
WHY DO WE CARE ABOUT DERMATOMES?
When trying to memorize all the spinal roots associated with each dermatome, it can be easy to lose sight of (or never really consider) WHY WE CARE IN THE FIRST PLACE ABOUT THE DERMATOMES. In reality, understanding these dermatomes can help us uncover the etiology behind what might be causing a neurological complaint a patient presents with.

In reality, a patient will come to the clinic with a constellation of neurological symptoms, and it will fall to the physician to collect “neurological clues” that can uncover what is behind the patient’s presentation. As far as “clinical clues” go, dermatomes are very useful in the sense that they can be traced back to a single spinal root, which can help localize where the issue may be in the nervous system.
HOW DO WE TEST THE FUNCTIONAL STATUS OF THE DERMATOMES?
While the rest of this page will cover specific dermatome locations/associated cranial nerve roots, let us first discuss UNIVERSALLY how one can correctly test if a dermatome is intact. It is for this reason that it is important to review how one can quickly and properly test a patients sensation on the skin. Let us quickly remember that there are 2 major sensory pathways that innervate these dermatomes: one pathway is responsible for light touch/sensing vibration/and proprioception, while the other is responsible for pain/temperature pathways. While there are a few different tools that can be used in the clinic to test sensation, the cotton swab is actually a very elegant option.

The beauty of the cotton swab is that it can be used to test both sensory pathways that innervate a dermatome. Once broken in half, the cotton side of the swab can test “light touch” while the broken end can be used to test pinprick. Given its cheap, sterile, and accessible nature, a cotton swab becomes our best friend in evaluating if dermatomes are intact.
DERMATOMES OF THE UPPER EXTREMITIES
When looking at the dermatomes that are found in the upper extremities we can see a pattern that really makes learning these dermatomes in this region very trivial!
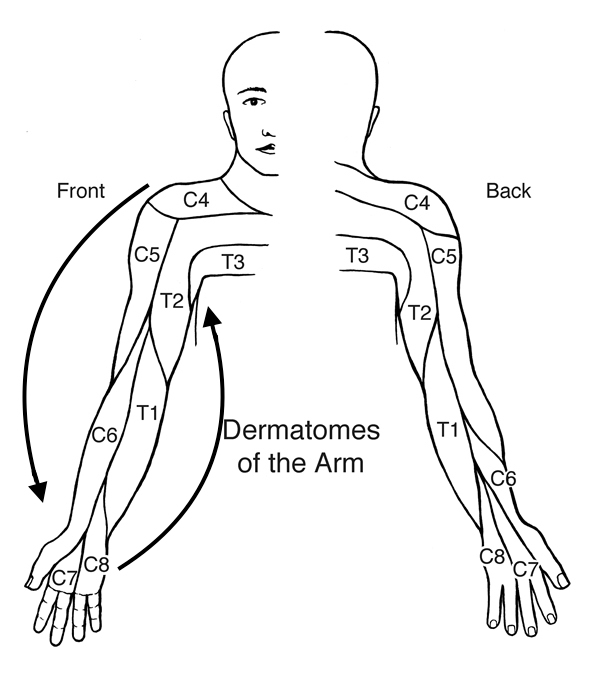
Where should we test for each spinal nerve? While the below locations are not the only areas of each spinal nerve dermatome (see the figure above) they are quick (and easy to remember) locations that can be tested rapidly in the clinic.
- C4 spinal root: upper shoulder (area around clavicle)
- C5 spinal root: lateral aspect of upper arm (such as lower deltoid)
- C6 spinal root: lateral aspect of lower forearm (thumb)
- C7 spinal root: mid palm (index finger)
- C8 spinal root: medial palm (pinky)
- T1 spinal root: lateral aspect of lower arm
- T2 spinal root: medial aspect of upper arm (medial portion of bicep muscle)
- T3 spinal root: armpit
DERMATOMES OF THE CHEST/ABDOMEN
The dermatomes of the chest/abdomen are very intuitive and really just follow a clear order.
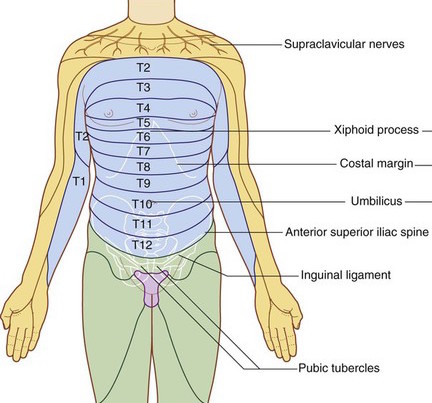
Some important landmark to keep in mind are:
- T4 spinal root: this dermatome is at the level of the nipple
- T10 spinal root: this dermatome is at the level of the umbilicus
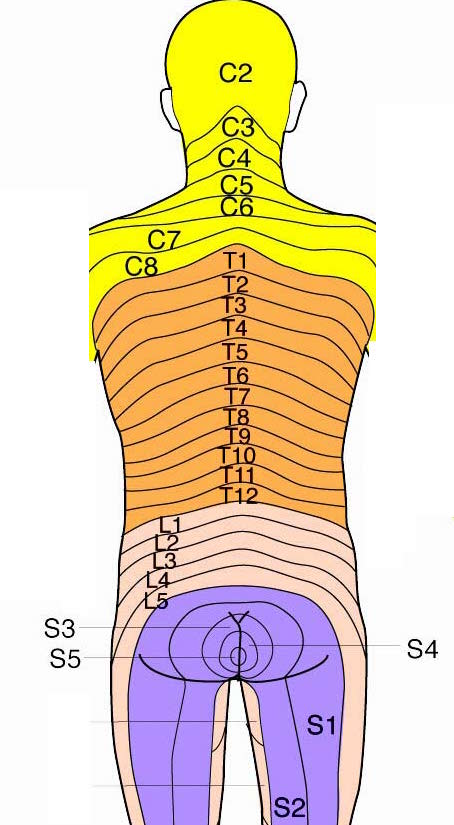
DERMATOMES OF THE BACK
The dermatomes of the chest/abdomen are very intuitive and really just follow a clear order.
DERMATOMES OF THE LOWER EXTREMITIES
Looking at the dermatomes of the lower extremity, again we can see a general pattern that might make it easier to remember the important spinal nerves.
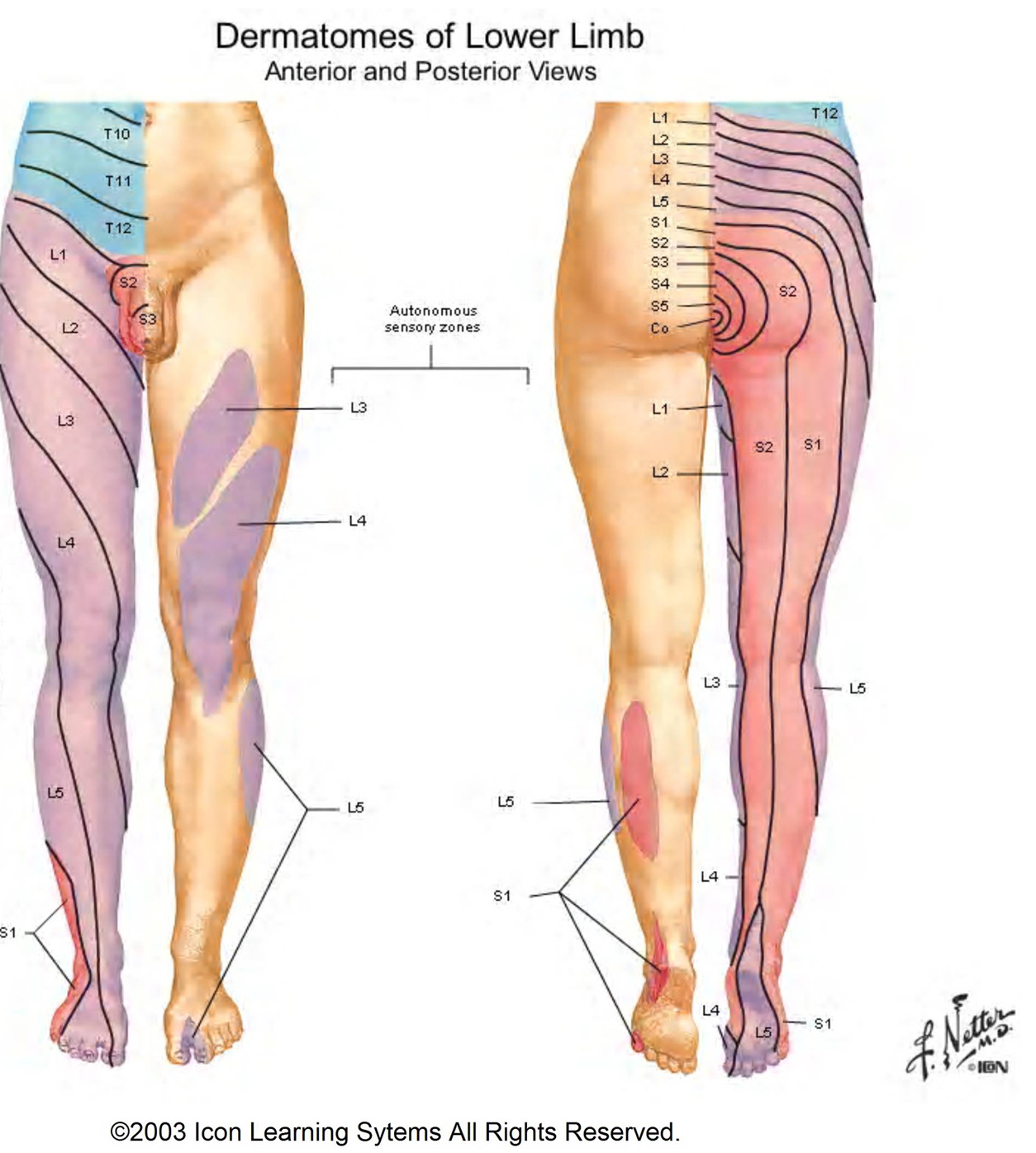
What are some important dermatomes that can be tested in the lower extremities? While there is not as clear of a pattern here as was seen with the upper extremities there are some important landmarks that we can test to evaluate the spinal nerves.
- L1 spinal nerve: inguinal ligament
- L2/L3 spinal nerves: upper thigh
- L4 spinal nerve: knee/large toe
- L5 spinal nerve: dorsal foot (first webspace)/ sole of foot (middle)
- S1 spinal nerve: lateral aspect of foot (pinky toe)/posterior lateral portion of leg
- S2 spinal nerve: posterior medial portion of leg
Page Updated: 10.02.2016