Page Contents
NEURAL PATHWAY
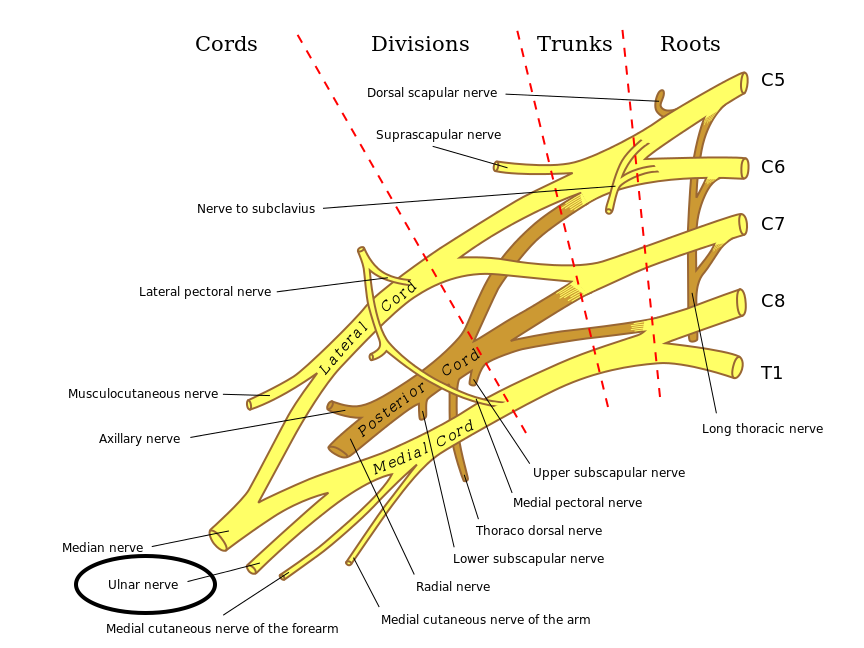
The ulnar nerve can be traced back to the spinal roots and follows the pathway outlined below to the periphery of the arm.
Branches of C8 and T1 (Sometimes C7) →Medial Cord (Brachial Plexus) → Ulnar Nerve
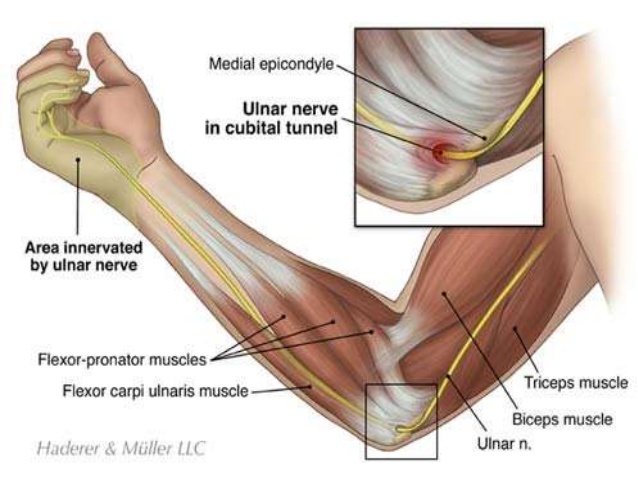
After leaving the brachial plexus the ulnar nerve will travel down the posterior/medial aspect of the upper arm and will pass through the cubital tunnel (which is located right near the medial epicondyle). From here the nerve will travel next to the ulnar bone (medial aspect of forearm) until reaching the wrist.
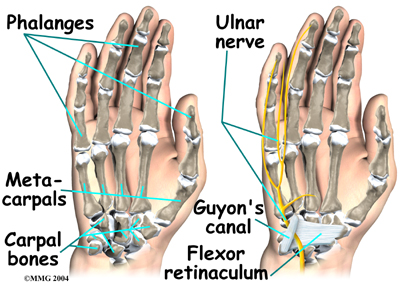
Upon reaching the wrist the ulnar nerve enters the palm of the hand via Guyon’s canal. From here it it innervates the palm of the hand and the ring/pinkey fingers.
Branches of the ulnar nerve include:
- Muscular branches
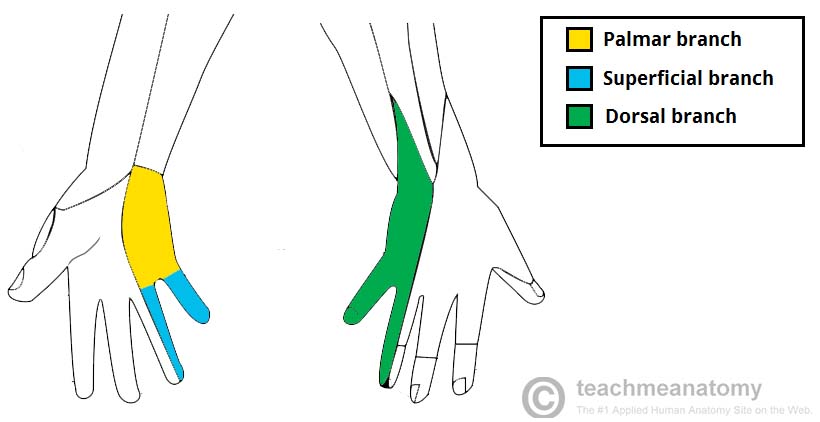
- Palmar branch
- Dorsal branch
FUNCTION
Motor (arm) via muscular branches:
- Medial deviation of hand: the ulnar nerve innervates the flexor carpi ulnaris muscle which flexes/adducts the hand
- Ring/pinky flexion: the ulnar nerve innervates the medial portion of the flexor digitorum profundus muscle.
Motor (hand) via deep branch:
- Pinky finger abduction: innervates the abductor digiti minimi
- Pinkey adduction: innervation of 3rd palmar interosseus muscle
- Controls opposition between pinkey and thumb by innervating the opponens digiti minimi muscle
- Pinky flexion via innervating the flexor digiti minimi brevis muscle
- Thumb adduction given that it innervates the adductor pollicis muscle
Sensory innervation (hand): different branches of the ulnar nerve will innervate both the posterior/anterior medial aspect of the hand (for sensory innervation). The tip of the pinky (palmar side) is exclusively innervated by the ulnar nerve.
CAUSE OF INJURY
Ulnar nerve entrapment at the elbow: this is the most common site of ulnar nerve entrapment.
Ulnar nerve entrapment at the Guyon canal: this nerve can also be trapped/compressed at the wrist.
CLINICAL PRESENTATION OF INJURY
Inability to adduct pinky: in some cases patients have a tonicly abductued little finger (Wartenberg’s sign)

{kind=link}
Ulnar claw can be present in patients who have long standing ulnar nerve damage. The ring and pinky fingers are hyperextended at the metacarpophalangeal (MCP) joint, and flexed at both interphalangeal (IP) joints.

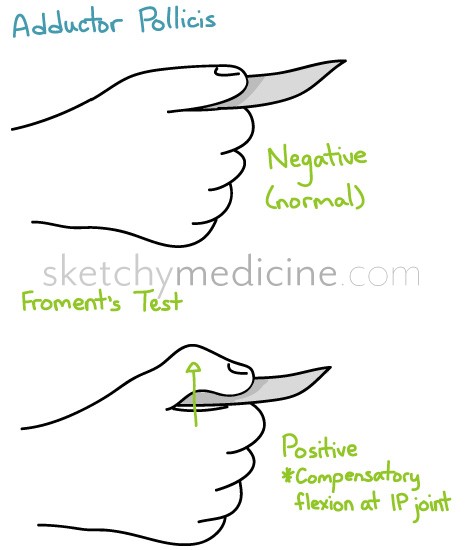
Froments sign can be positive in patients with ulnar nerve palsy. With ulnar nerve palsy patients can’t hold onto items tightly between their thumb and forefinger without flexing their flexor pollicis longus muscle (causing a visible “pinching”). This pinching during the test is referred to a positive Froment’s sign.
OTHER INFO
Nerve conduction studies/EMG can be used to evaluate if the ulnar nerve is intact (given suspicion of ulnar nerve palsy/damage).
ARCHIVE OF STANDARDIZED EXAM QUESTIONS
This archive compiles standardized exam questions that relate to the injury of this nerve.
Page Updated: 06.19.2016