Page Contents
OVERVIEW
The purpose of this page is to take the notable study titled “Detection Of Subarachnoid Hemorrhage On Early CT: Is Lumbar Puncture Still Needed After A Negative Scan?” (Van Der Wee & Rinkel et al. 1995, Journal of Neurology, Neurosurgery, and Psychiatry) and distill down its major takeaways for clinical practice.
WHAT IS THE POINT OF THIS STUDY?
The overall purpose of this study was to evaluate and see if a CT scan alone was sufficient to detect a subarachnoid hemorrhage, or if this study should be supplemented with a lumbar puncture.
WHAT IS THE CLINICAL STRUGGLE?
While relatively rare (~30,000 cases per-year in the U.S.), subarachnoid hemorrhages (SAH) are often life-threatening. Mortality rates from SAH vary from 20-45% in the literature, with many surviving patients severely disabled. Rebleeds are a common cause of death from SAH and are most likely to occur within 6 hours of the initial bleed, making early detection and treatment of SAH vital. CT scans are not 100% sensitive for SAH, patients with a negative CT may need to be supplemented with a lumbar puncture (LP) in order to detect certain cases of SAH. LPs are not specific until 12 hours after the bleed; before that time true positives cannot be distinguished from traumatic taps.

WHAT ARE THE MAJOR TAKEAWAYS?
Overall:
- Because of the importance of early detection of SAH in patient outcomes, the authors wanted to know if a CT scan without an adjunctive lumbar puncture is sufficient for diagnosis in patients suspected of having SAH.
- In retrospective analysis of 175 patients admitted for severe headache, a CT scan within 12 hours of headache onset detected 117 out of 119 subarachnoid hemorrhages. SAH was confirmed in the two cases with normal CTs by both lumbar puncture and angiography. Thus, CT alone is insufficient for detecting SAH.
- Patients with normal CT scans within 12 hours of severe headache onset should be admitted until a lumbar puncture performed 12+ hours after onset rules out SAH.
WHAT WAS THE STUDY POPULATION USED?
The study sample was 175 patients with sudden onset severe headache presenting to two hospitals in the Netherlands between 1989-1993. In the sample there were 119 confirmed cases of SAH, with two of those cases having a negative CT.
All patients had a non-contrast CT (within 12 hours of their headache onset) read by one neuroradiologist and two neurologists. All patients with a CT negative for SAH underwent a lumbar puncture at least 12 hours after headache onset. LPs were positive for SAH (meaning blood and xanthochromia were present) in two patients; angiography confirmed SAH in these cases.
WHEN WAS A CT SCAN NOT ENOUGH?
In this study, the CT scan missed SAH in 2 of 119 cases. 12 hours after headache onset, LP was able to detect those cases.
In looking at this study (as well as others) the table below summarizes the sensitivity and specificity of both a non-contrast CT-scan and lumbar puncture for the deletion of SAH:
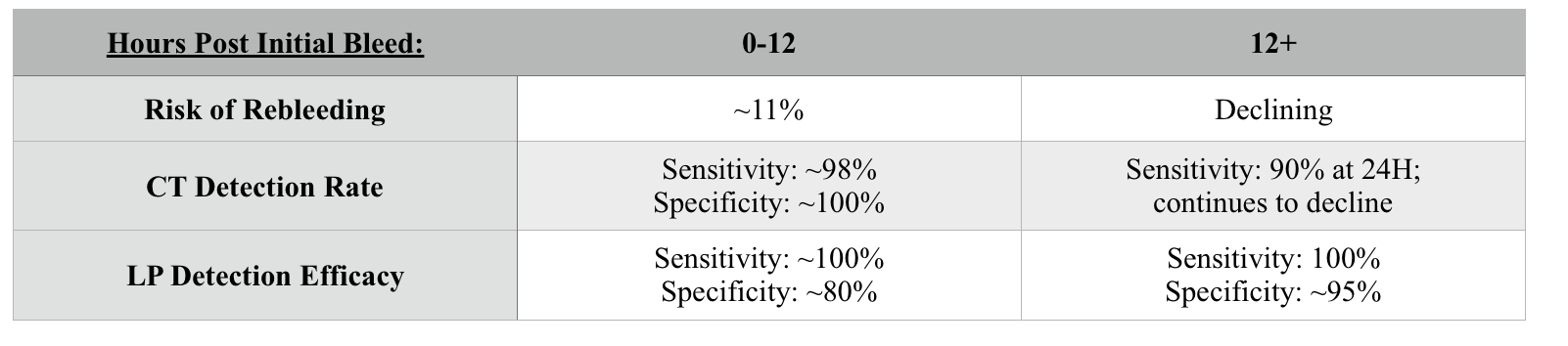
WHAT CAN WE CONCLUDE?
Within 12 hours of headache onset, non-contrast CT alone cannot detect 100% of SAHs. Because of the poor prognosis of untreated SAH, patients presenting with severe headaches should be admitted for at least 12 hours post onset until an LP can be performed to rule out SAH.
The results of this paper are still true today. Even with newer CT scanners, LP after a negative CT is recommended.
FURTHER READING
Given that this study was published a while ago, this paper (Detection of subarachnoid haemorrhage on early CT: is lumbar puncture still needed after a negative scan?) is recommended as a source of further reading)
CITATIONS
The following sources were used to create the information on this page:
- Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage
- Rebleeding, secondary ischemia, and timing of operation in patients with subarachnoid hemorrhage
- Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage
- Detection of subarachnoid haemorrhage on early CT: is lumbar puncture still needed after a negative scan?
- Incidence of Traumatic Lumbar Puncture
- Distinguishing traumatic lumbar puncture from true subarachnoid hemorrhage
- Interpreting Red Blood Cells in Lumbar Puncture: Distinguishing True Subarachnoid Hemorrhage From Traumatic Tap
- Lumbar puncture and the diagnosis of CT negative subarachnoid haemorrhage: time for a new approach?
- Subarachnoid hemorrhage diagnosis by computed tomography and lumbar puncture: Are fifth generation CT scanners better at identifying subarachnoid hemorrhage?
Page Updated: 12.05.2017