Page Contents
OVERVIEW
This page is dedicated to organizing various examples of standardized exam questions whose answer is hereditary spherocytosis (HS). While this may seem a odd practice, it is useful to see multiple examples of how hereditary spherocytosis will be characterized on standardized exams (namely the boards and the shelf exams). This page is not meant to be used as a traditional question bank (as all of the answers will be the same), however seeing the classic “test” characterization for a topic is quite valuable.
KEY CHARACTERISTICS OF THIS CONDITION (ON EXAMS)
When it comes to standardized exams, each topic has its own “code” marked by key buzzwords, lab findings, clues, etc. If you are well versed in this code you will be able to more quickly identify the condition that is being discussed, and get the right answer on the exam you are taking. Below is the “code” for hereditary spherocytosis.
Chief Complaints:
- Jaundice may be observed by the patient
- Symptoms of anemia: fatigue, pallor, etc.
Clinical Workup:
- Signs of jaundice can be detected on the physical exam (scleral icterus, yellowed skin).
- Skin pallor/signs of anemia can be detected on the physical exam.
- Splenomegaly can be detected on physical exam.
- Signs of hemolytic anemia: patients will often have anemia detected on a CBC. This often times will present in the setting of a suspected hemolytic anemia (such as in the presence of elevated LDH, elevated indirect bilirubin).
- Normal liver enzymes: bilirubin is not elevate due to any liver pathology in this case.
- MCHC will be increased in this condition (very specific)
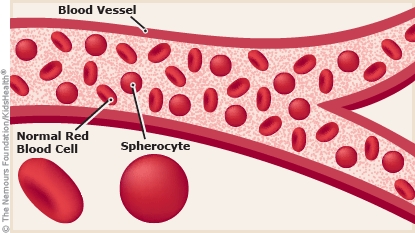
- Spherocytes can be seen on a blood smear (look for very spherical RBCs with no central pallor)
- Negative Coombs test as this is not a antibody mediated condition.
- Increased osmotic fragility: cells will lyse easily in hypotonic solution (releasing hemoglobin). This helps to make the diagnosis.
QUESTION EXAMPLES
Question # 1
A 22 year old male comes in for evaluation of recurrent episodes of jaundice. His past medical history is non-contributory otherwise. Currently his vital signs are within normal limits. A physical exam reveals splenomegaly, skin pallor, and scleral icterus. The remained of the physical exam is within normal limits. Labs are collected and are shown below:
- Hemoglobin: 8.7 g/L ***
- Platelet count: 200,000/mm³
- WBC: 6300/mm³
- LDH: increased ***
- Total bilirubin: 3.5 mg/dL
- Diret bilirubin: 0.3 mg/dL
- Liver enzymes: WNL
- Direct Combs test: negative
The patients red blood cells are incubated in a hypotonic solution (containing glycerol) and it is noted that hemoglobin levels increase in the sample (relative to controls that do not release hemoglobin). What is the likely diagnosis in this patient?
Explanation # 1
Jaundice + hemolytic anemia (LDH increased) + positive osmotic fragility test = hereditary spherocytosis
Question # 2
A 17 year old male comes to the clinic because he has recently noticed that his skin is more yellow then before. His past medical history is otherwise unremarkable. A physical exam is notable for jaundice. Lab studies are conducted and reveal anemia, a high reticulocyte count, and elevated indirect bilirubin. A peripheral blood smear is performed and is shown below:
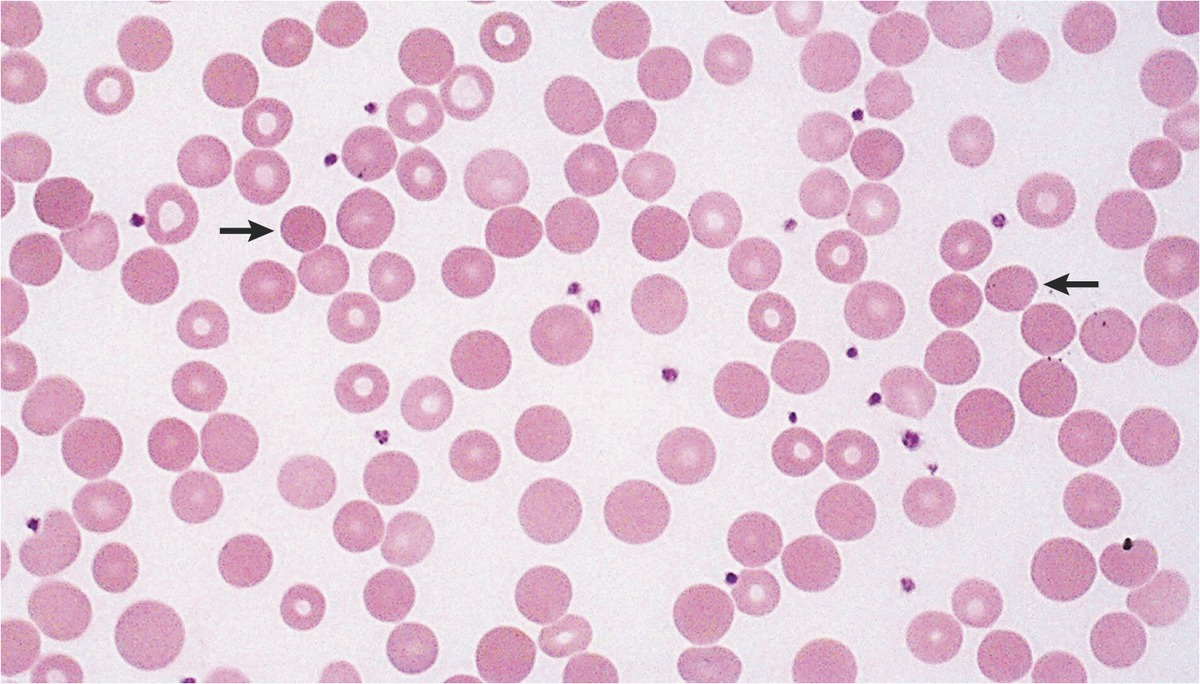
What is the likely diagnosis in this patient?
Explanation # 2
Jaundice + hemolytic anemia (elevated indirect bilirubin) + spherocytes on blood smear = hereditary spherocytosis
Question # 3
A 12 year old female is brought to the clinic because she is fatigued and appears pale. Her family history is notable for a father who underwent a splenectomy for persistent anemia, and recently underwent a cholecystectomy. Lab values are shown below:
- Hemoglobin: 6.7 g/dL ***
- MCV: 90 µm³
- WBC count: 6200/mm³
- Platelets: 190,000/mm³
- Reticulocyte count: 8% of red cells (N = 0.5-1.5 %)
A blood smear is performed and shown below.

What is the likely diagnosis in this patient?
Explanation # 3
Anemia + spherocytes on blood smear = hereditary spherocytosis
Question # 4
A 20 year old female comes to the clinic because she has been experiencing fatigue recently, and has noticed that her eyes have turned yellow. Her past history is notable for a mild anemia, but is otherwise unremarkable. Currently her temperature is 98.1°F, pure is 80 bpm, and her blood pressure is 110/70 mm Hg. A physical exam is notable for scleral icterus and splenomegaly. Lab studies are shown below:
- Hemoglobin: 8.5 g/dL ***
- MCHC: 39% Hb/cell ***
- Reticulocyte count: 8 %
- Serum total bilirubin: 3.2 mg/dL
A direct Coombs test is performed and is negative. A blood smear is performed and shown below:
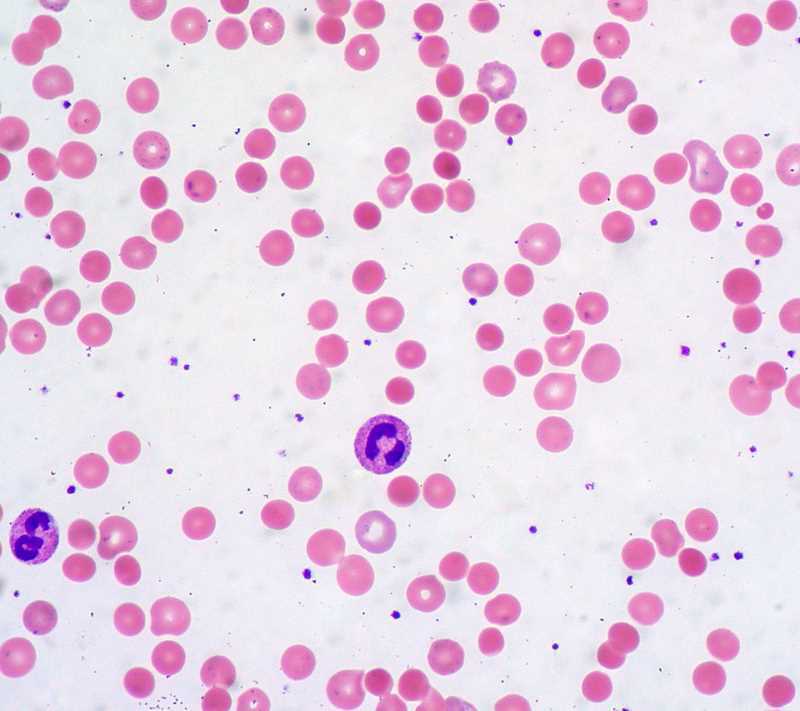
What is the likely diagnosis?
Explanation # 4
Anemia + elevated MCHC + spherocytes on blood smear = hereditary spherocytosis
TESTABLE FACTS ABOUT THIS TOPIC (BEYOND ITS IDENTIFICATION)
Many questions on standardized exams go beyond simply recognizing the underlying topic. Often there are specific testable facts regarding some aspect of the topic’s pathophysiology/management/clinical implications that are commonly asked. Some of these are listed below:
Cause:
- Cause: Red blood cell membrane defect caused by mutations involving spectirn and ankyrin (plasma membrane scaffolding proteins).
- Inheritance pattern: autosomal dominant (most of the time)
Management:
- Treatment: splenectomy is usually curative
Other:
- Complications: pigmented gallstones, aplastic crisis from parvovirus infection.
Page Updated: 03.27.2018