Page Contents
OVERVIEW
This page is dedicated to covering the important aspects of the newborn physical exam. It is separated into the major components of the exam (in the order that is optimal given that the baby is quietest at the beginning of the exam).
RESPIRATORY SYSTEM
Color: a good sign of proper oxygenation and perfusion is if the baby (and its extremities) are a reddish pink.
Respiration: there should be no expiratory grunting heard and no flaring of the alae nasae seen.
Respiration rate: A normal respiratory rate is under 60. Many newborns are periodic breathers. They will breathregularly for a minute or two, but then with a short period of no breathing at all (usually 5-10 seconds). While this is the case, apnea (periods of no breathing during which an infant’s color changes from the normal reddish-pink to grades of cyanosis) is not a normal phenomenon for a full term baby.
Respiratory auscultation: Stridor should not be heard with inspiration. Occasional rales may be heard.
CARDIAC SYSTEM
Heart rate: a normal pulse in a newborn is 120-160.
Hear auscultation: heart sounds should get louder on the left. Murmurs early in life (i.e. first day of life) may go away after 2-3 days.
Pulses: brachial and femoral pulses can be palpated.
ABDOMEN
Visaul Inspection: are there apparent masses, asymmetry, or discoloration?
Palpation: if needed the knows can be flexed up to the abdomen to relax the abdominal muscles. Palpate for the spleen and liver. Fetal ultrasound is usually more informative than this component of the physical exam.
GENITALIA/RECTUM
Inspection: both male/female genitalia should be inspected for abnormalities. The rectum should be checked for patency, position, and the absence of fistulas.
In males The testes should be palpated bilaterally to ensure that they have properly distended.
SKIN
It is important to assess not only for cyanosis (as was done earlier) but also for any rashes, suspicious nevi, or jaundice.

EXTREMITIES, SPINE, AND JOINTS
Inspect for any obvious abnormalities of the digits (too few/too many) and for club feet.

{kind=link}
Hip dislocation can be easily missed if not tested for appropriately:
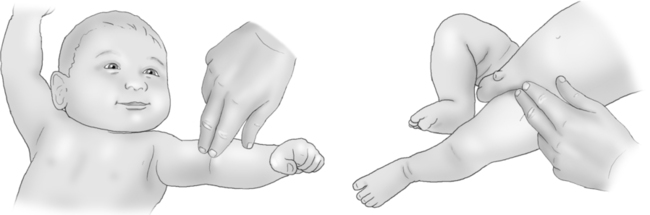
- The Galeazzi exam tests for unilateral hip dislocation by comparing the knee height when the legs are flexed so the heals meet the buttocks (they are symmetrical if none, or both legs are dislocated)
- The Ortolan exam can test for hip dislocation bilaterally (one at a time).
- The Barlow exam can test for a more rare form of hip dislocation bilaterally.
The lower spine should be evaluated for any obvious spinal defects.

HEAD/NECK/MOUTH
The head should be carefully examined for any abnormalities. The normal limits of head circumference are ~ 33-38 cm. First born infants (usually having undergone much longer labors), often have very prominent molding of their occiputs with accompanying sloped foreheads. This is temporary. The size of the anterior fontanel is ~5-6 cm.
The neck of an infant is difficult to visualize and requires elevation of the chin. Check for structural abnormalities, goiters, or issues with range of motion.
The mouth should be checked for any abnormal pathology (such as cysts, clefts, etc.)
EYE EXAM
Using an opthalmascope, one can check for the “red reflex” in the eyes of the newborn (which can reveal cataracts or retinoblastoma).

NEUROLOGICAL EXAM
The neurological exam can become extensive for the newborn. Here are some of the different tests that can be done (but are not always done).
Rooting test: the rooting test is performed by stroking the upper lip of the newborn. Usually newborns will turn their mouth toward the stimulating finger, thinking that they will be able to suckle it.
Suckling: putting your gloved finger in the mouth should elicit a strong suckling response by the newborn.
Grasp: putting your finger in the baby’s palm and pressing down should cause the baby to grasp strongly.
Moro test: this is performed by lifting the infant slightly off their resting surface (by their arms) and then letting them drop. This startles the baby and should result in the baby throwing their arms straight out, opening their fingers wide, flexing their legs, curling their toes and then sometimes letting out a scream.

Babinski sign: in newborns scraping the bottom of the foot will lead to an up-going babinksi response (large toe pointing upward).

MEAUREMENTS
These measurements usually are the final parts of the exam.
- Weight: The normal weight of a full term (38-42 week) infant is 2.5-4 kg
- Head circumference: ~33-38
- Length: 19-21 inches
Page Updated: 05.15.2016