Page Contents
OVERVIEW
This page is meant to discuss more about how to protocol a Right Upper Quadrant Ultrasound (Gall Bladder And Ducts) radiology imaging study. This page is meant to be used both by both those inside and outside the field of radiology to better appreciate the utility of this imaging study, and when best to order it.
WHAT DOES THIS STUDY ACTUALLY INCLUDE?
When you are protocoling/ordering this study it is important to realize exactly what you are “getting” from the study. This is what a typical right upper quadrant ultrasound protocol entails:
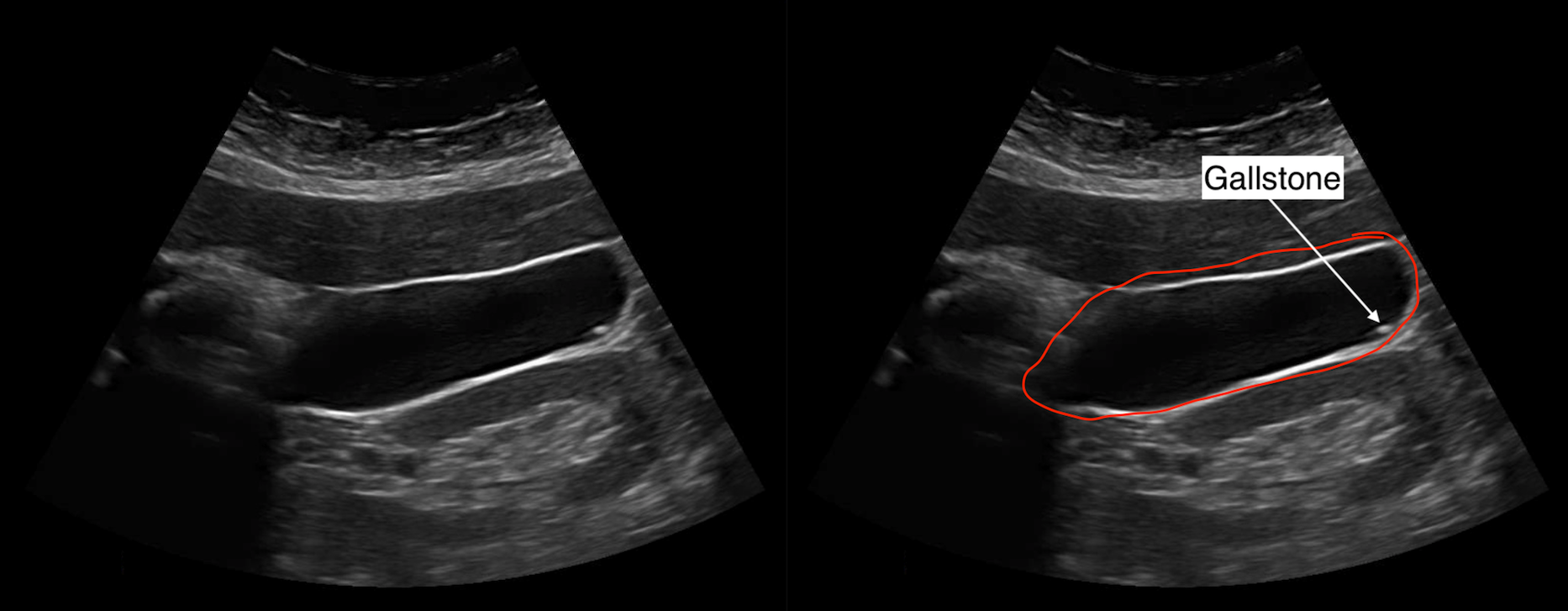
- Full evaluation of the gall bladder: a central part of the study is to fully evaluate the gall bladder. This means multiple orientations, and views of the entire organ (both still images and cine clips).
- Sonographic Murphy’s sign: as the technologist preforms their scan, they take special note if the patient’s abdominal pain is the worst when they are scanning with the probe over the gall bladder. If it is, the sonographic Murphy’s sign is said to be positive.
- Common bile duct: a portion of thee common bile duct is visualized, and its size is measured at the level of the porta hepatis.
- Limited view of the main portal vein: the main portal vein is typically partially visualized and used as a landmark to find the common bile duct. A doppler image showing flow in the portal vein is acquired, and a spectral wav form may also be acquired.
- Limited view of the liver parenchyma: portions of the liver will be imaged adjacent to the gall bladder and some intrahepatic pathology may be visualized (such as intrahepatic biliary dilatation) however typically a RUQ ultrasound does not fully evaluate the liver.
WHEN SHOULD THIS STUDY BE ORDERED?
It is important to appreciate that a right upper quadrant ultrasound really is best for evaluating the gall bladder and the biliary system. In the majority of cases this study is ordered to help make the diagnosis of cholecystitis when there is appropriate clinical concern. There are a few common scenarios that will be clear indications for ordering this study (some of which are overlapping):
- Physical exam concerning for cholecystitis: right upper quadrant pain (typically colicky in nature)
- Lab abnormalities concerning for cholecystitis: elevated liver enzymes (especially alk phos) and bilirubin may be present.
- Questionable appearance of the gall bladder on other imaging studies: patients may receive other imaging studies (such as abdominal CT or MRI) for their workup. In certain cases the appearance of the gallbladder may prompt the radiologist to recommend further evaluation with ultrasound.
WHEN SHOULD THIS STUDY NOT BE ORDERED?
While it may be hard to find true absolute contraindications for performing a right upper quadrant ultrasound, there are a few cases in which the study should probably not be ordered:
- In patients who have recently eaten: in the post prandial state, the gall bladder becomes contracted and its evaluation is limited. Often times a RUQ ultrasound for cholecystitis will be non-diagnostic in this post-prandial state (findings like wall thickening can not be interpreted clearly as they may be the artifact of normal post-prandial contraction). Keeping the patient NPO for at least 8 hours is generally preferred (however sometimes shorter time points like 4 hours may be acceptable).
- In patients who have recently received pain medication (such as opioids): patients with complaints of abdominal pain may have already received pain medication which can complicate the interpretation of the Sonographic Murphy’s sign. In the absence of being able to evaluate for this sign, often times the ultrasound is non-diagnostic for cholecystitis.
- In patients with a past cholecystectomy: While the gallbladder is not the only thing imaged during this study, it in many ways is the focus of the study. In patients who don’t have a gall bladder the yield of the study can be questionable.
- In patients who have a broader differential for their presentation: while a RUQ ultrasound is very helpful for evaluating for specific diagnoses like cholecystitis, in cases where the suspected differential is broad (such as in the case of generalized abdominal pain) this study may be too limited. It is sometimes important to consider if other studies (like a CT scan of the abdomen and pelvis with IV contrast) may be more appropriate and useful in working up the patient.
WHAT ELSE SHOULD BE ORDERED WITH THIS STUDY?
When ordering this imaging study, here are a few other orders to consider so that one gets the most the out right upper quadrant ultrasound:
Orders to increase the chance of a diagnosis:
- NPO diet order: to prevent the gall badder from being difficult to evaluate, the patient should be kept NPO prior to the ultrasound study (ideally 8 hours, however shorter time points are sometimes OK such as 4 hours in certain circumstances). Also in general patients who are being worked up for cholecystitis should not be eating
- Discontinue pain medications (especially opioids): one of the most important components of a RUQ ultrasound is evaluating for a Sonographic Murphy’s sign. In patients who have their pain masked by medications, this sign can not be assessed if it is negative, which limits the value of the study.
Complementary diagnostic testing:
- Liver function tests (including bilirubin): while often times LFTs and bilirubin may be normal in patients with cholecystitis, sometimes these lab values can be helpful for working up the patient and conteextualziing findings of a right upper quadrant ultrasound.
Page Updated: 01.12.2020