Page Contents
OVERVIEW
This guide is designed to help make it more simple to replete electrolytes. The major electrolytes that we will be covering are:
- Magnesium (target 2.0 mEq/L)
- Phosphate (target 3.0 mEq/dL)
- Potassium (target 4.0 mEq/L)
REPLEATING MAGNESIUM (MAG)
Let us keep in mind that our target level is 2.0 mEq/L. How below we are this target concentration will dictate the dose that we give:
- 1 gram IV generally increases the serum value by 0.1 mEq/L
Patients with a serum magnesium of 1.5 – 2.0 mEq/L:
- 2 grams Magnesium Sulfate IV over 1 hour
- No additional followup/monitoring needed
Patients with a serum magnesium of 0.9-1.4 mEq/L:
- 4 grams Magnesium Sulfate IV over 2 hours
- Recheck serum magnesium level 2 hours after infusion is complete
Patients with a serum magnesium of < 0.9-1.4 mEq/L:
- Let more senior physician know how low Mag is.
- 4 grams Magnesium Sulfate IV over 2 hours
- Recheck serum magnesium level 2 hours after infusion is complete
PO Magnesium Should Be Avoided Because It Upsets The GI System
- Ok to use if diarrhea is desired
- 400mg PO BID x 2-5 days for Mg 1.8mg/dL,
- 400mg PO TID x2-5 days for Mg 1.6-1.7mg/dL
- 800mg PO BID x 2-5 days for Mg 1.4-1.6.
- Give IV magnesium if lower than 1.4.
REPLEATING PHOSPHATE (PHOS)
For patients with Renal Disease!
Be mindful of repleting phos. Patients with ESRD on HD and urine output should likely not replete without a renal consult.
There are 2 major types of IV phos:
- Potassium Phosphate: give to patients who also have low potassium or high sodium.
- Giving 15 mmol of KPO4 will give 13.2 mEq of K. Factor that in when repleting K.
- Sodium phosphate: give to patients with a serum potassium > 4.5mEq/L and serum sodium <145 mEq/L sodium.
Let us keep in mind that our target level is 3.0 mEq/dL. How below we are this target concentration will dictate the dose that we give:
Patients with a serum phosphate of 2 – 2.5 mEq/dL:
- 15 mm potassium phosphate IV over 4 Hrs
- No additional followup/monitoring needed
Patients with a serum phosphate of 1 – 1.9 mEq/dL:
- 21 mm potassium phosphate IV over 4 Hrs (or 30 mm phosphate over 4 hours?)
- Recheck serum phosphorous level 2 hours after infusion is complete
Patients with a serum phosphate of < 1 mEq/dL:
- Let more senior physician know how low Phos is.
- 30 mm phosphate over 4 hours (or 40 mm phosphate over 6 hours?)
- Regardless, after giving 30 mmol recheck serum phosphorous level 2 hours after infusion is complete and then add more as necessary.
Giving PO Phos:
For phos 2.2mg/dL or greater without significant medical issues related to phos alterations and taking POs, use Neutra-phos packets.
Generally use gestalt for this and don’t calculate. The following works: give 2 packets Neutra-Phos TID with meals x1-2 days for phos 2.2-2.4mg/dL or 1 packet TID with meals for phos 2.5-2.7mg/dL
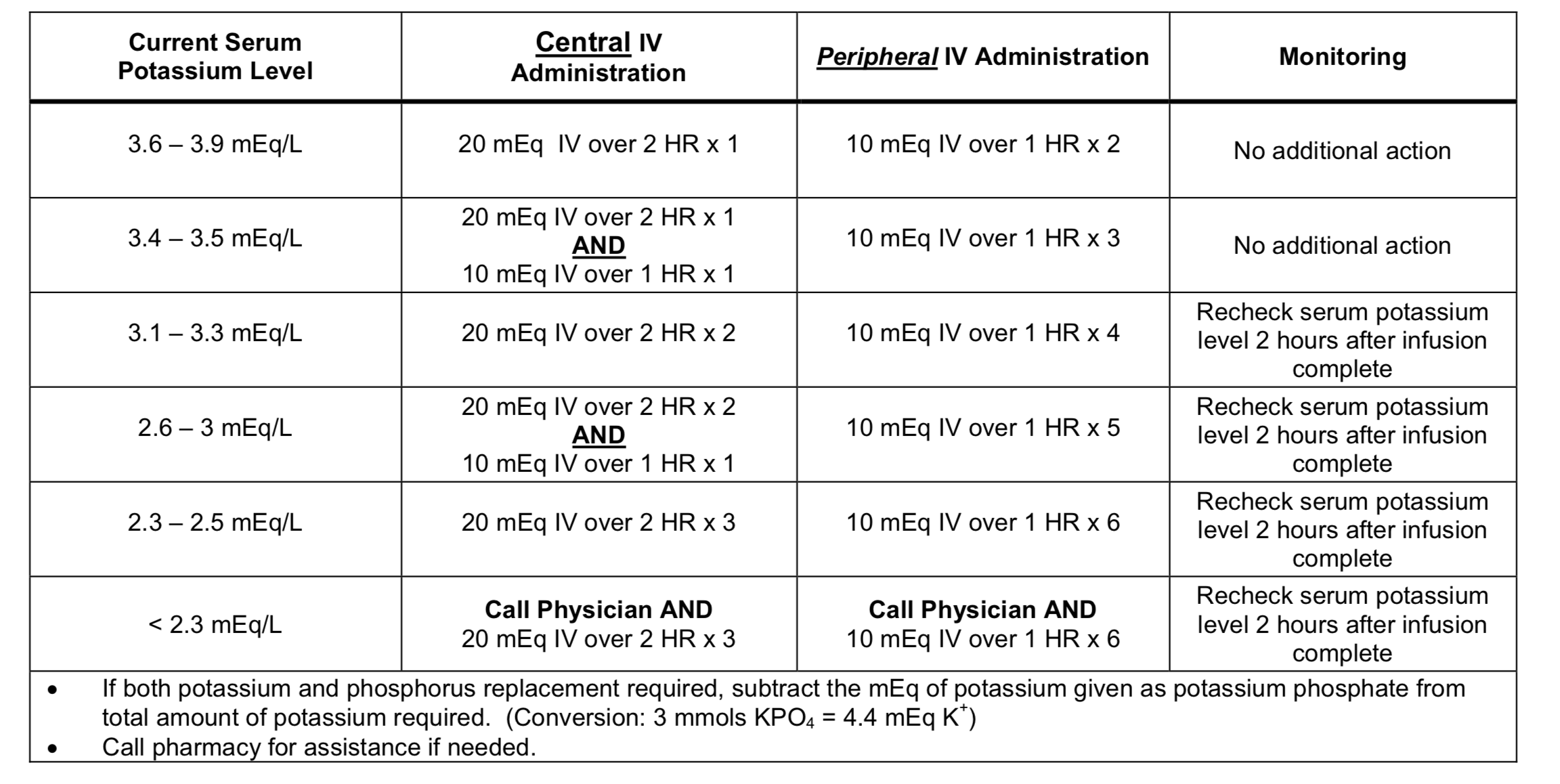
REPLEATING POTASSIUM (K)
Generally given 10 mEq IV should increase value by 0.1 mEq/L
Two concentrations of IV delivery:
- Central: 20 mEq/50 mL
- Peripheral: 10 meEq/50mL
Let us keep in mind that our target level is 4.0 mEq/dL. How below we are this target concentration will dictate the dose that we give:
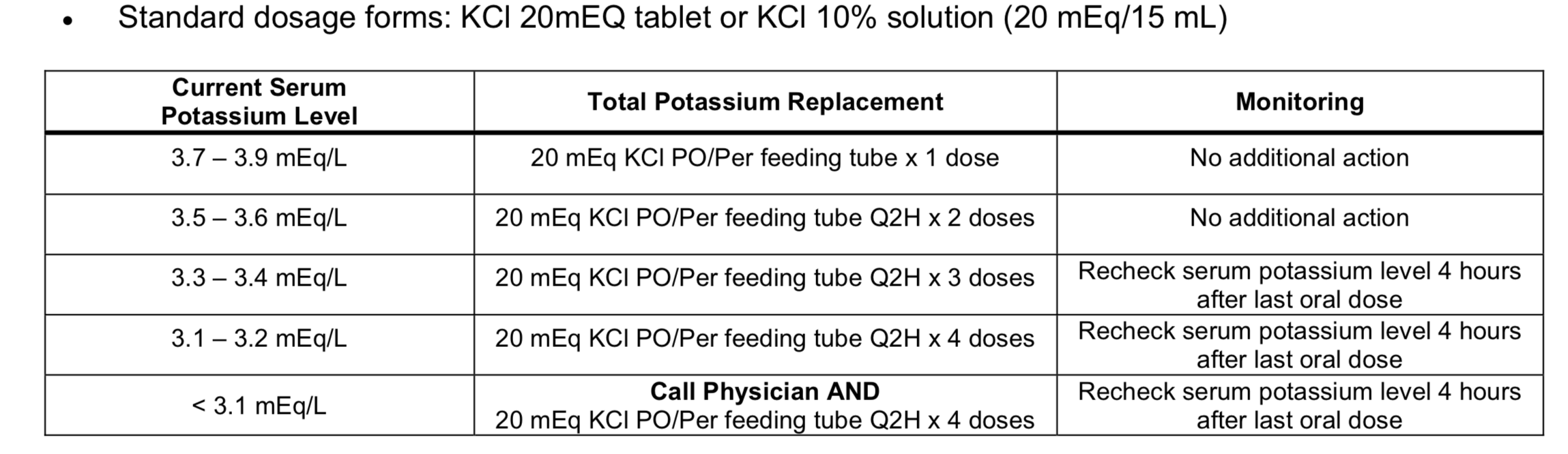
PO Potassium:
Page Updated: 06.19.2018