Page Contents
WHAT IS IT?
Autosomal dominant polycystic kidney disease (ADPKD) is an autosomal dominant genetic condition that is characterized by either a mutation in the PKD1 gene (most cases, on chromosome 16) or the PKD2 gene (chromosome 4). This PKD presents in adolescents/adults unlike ARPKD which is seen in neonates/young children.
WHY IS IT A PROBLEM?
Mutations in these genes ultimately cause a generalized abnormality of collagen. This results in the formation of numerous cysts on the kidneys causing their destruction and enlargement (eventually leading to renal failure). Death can occur from complications associated with chronic kidney disease or hypertension (increased renin production as a result of kidney damage).
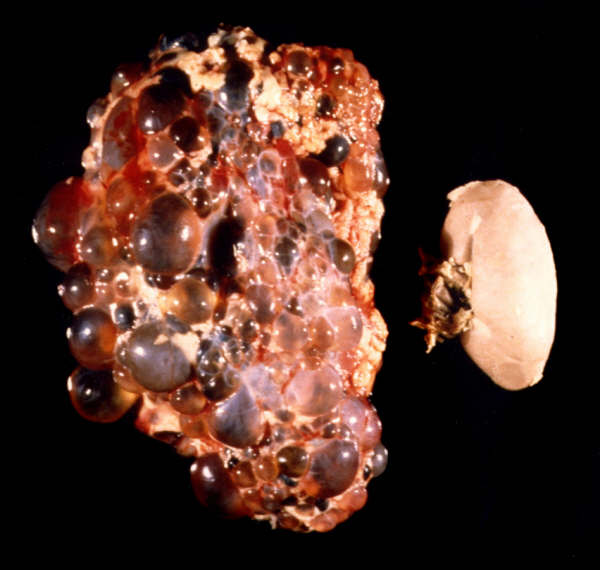
Whats more, these cysts can rupture leading to peritonitis/flank pain (if cysts were outside the kidney) or hematuria (if cysts ruptured in the renal pelvis)
Other organs are affected because this is a generalized collagen defect (see more in the “What else are we worried about?” section).
WHAT MAKES US SUSPECT IT?
Risk factors: family history
*Many patients can be asymptomatic
Hematuria caused by rupturing of cysts in the renal pelvis. Usually macroscopic.
Flank pain (or lower back) caused by rupturing of cysts outside the kidney
Hypertension as a result of kidney disease/damage (increased renin signaling)
Severe headache/loss of consciousness may indicate a ruptured intracranial hemorrhage.
Urinary tract infection symptoms are also common due to increased risk of developing a UTI with this condition (frequency, urgency, painful urination)
HOW DO WE CONFIRM A DIAGNOSIS?
Urine analysis can reveal the presence of both protein and blood (RBCs) in the urine. *Make sure to measure creatinine/GFR to assess for kidney failure (and have a baseline for the patient)
Renal ultrasound is very useful for diagnosing this condition.

Genetic testing can identify the casual mutatoin and give a definitive diagnosis of ADPKD
HOW DO WE RULE OTHER DIAGNOSES OUT?
The renal ultrasound (before conducting a renal biopsy for suspected nephritic conditions) can be useful in eliminating other diagnosis.
HOW DO WE TREAT IT?
No treatment currently exists that can slow disease progression/kidney damage. Treatment is instead geared towards the manifestations of the condition which include:
- Pain: acetaminophen and other analgesics used
- Hypertension: ACE inhibitors/ARBs
- Cyst infection: antibiotics
- End stage renal disease: dialysis or transplantation
HOW WELL DO THE PATIENTS DO?
This is a progressive disease that can not be stopped with any current medical intervention. As the patient grows older cysts increase in size and number.
WAS THERE A WAY TO PREVENT IT?
This genetic condition is not preventable.
WHAT ELSE ARE WE WORRIED ABOUT?
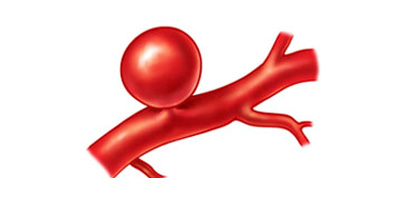
Berry (saccular) aneurysms are thin walled arterial outpouchings that lack a media layer, and are at risk for rupture. These can be caused by wall weakening/collagen defect (as seen in ADPKD) .
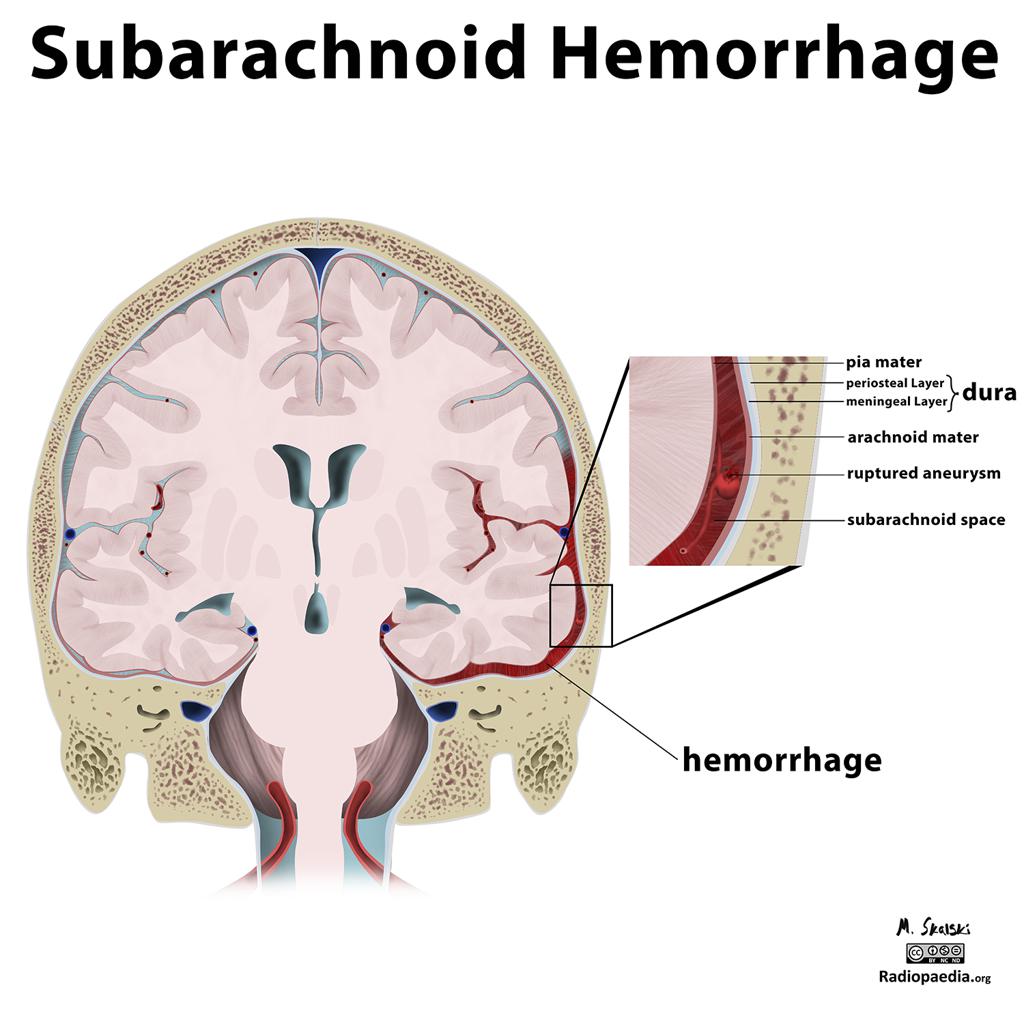
Subarachnoid hemorrhage: due to the formation of berry aneurysms, this type of hemorrhage (“worst headache of my life”) is associated with ADPKD.
Mitral valve prolapse can be caused by valvular collagen abnormalities in ADPKD
Benign hepatic cysts are also associated with ADPKD
Weakening of colonic wall is also observed due to collagen abnormalities.
OTHER HY FACTS?
Formerly called adult polycystic kidney disease
Most common inherited cause of kidney disease
FURTHER READING
Page Updated: 02.10.2016